Therapy is a powerful tool that anyone can benefit from – it can help with personal growth, healing, self-discovery and compassion towards both yourself and others. Yet, despite more and more people speaking about therapy and what it entails, there are still myths surrounding it which can cause hesitation and doubts about whether it is something to consider.
Therapy is only for people with ‘serious’ mental health issues:
Therapy isn’t just for those with severe mental health issues or those in crisis. It is a resource that can be used by anyone facing life challenges, seeking personal growth, or wanting to understand themselves better. I had a Psychology teacher when I was studying for my A Levels who told me that she really strongly believed that everyone, mental health conditions or not, should have to have therapy at some point in their life – and looking back, I absolutely agree!
Talking to friends and family is just as effective as therapy:
I am absolutely NOT wanting to dismiss the invaluable support that friends and family can offer you – I have incredible support from my family and friends and I wouldn’t be able to do life without them by my side. Therapy, however, offers something different. Therapists are trained professionals who are there in a neutral, non-judgemental capacity. They use evidence-based techniques to help you process emotions, identify patterns, and develop coping strategies.
Therapy takes forever to work:
How long therapy takes to work is entirely dependent on your goals and needs. Some people find huge benefits within a few weeks, whereas others benefit more from long-term work. It’s something to discuss with your therapist as they are in the best position to help you determine what is best for you.
The therapist will judge me or think that I am broken beyond repair:
Therapists are there to provide empathy and understanding, not to judge you. They aren’t there because they think you are broken and need fixing – they just want to help you work towards your goals in a partnership with you.
Therapy is all about your childhood experiences:
For some people, talking about their childhood is absolutely necessary. And for most people, looking at past experiences can be helpful, but therapy isn’t solely focused on the past/your childhood. The therapeutic process should be tailored to address your current concerns, whether they stem from past or present experiences.
My therapist will solve my problems for me:
As nice as this would be, it’s simply not possible for the therapist to do the work for you. Ultimately, change has to come from you – the therapist can help you and give suggestions and guidance, but you have to be the one to make those changes. One of my most commonly used phrases in my therapy sessions used to be “but I’m paying you to agree with me” which would inevitably result in an eye roll and being reminded that she definitely is NOT there to agree with me – it would be nice if she did, but then no progress would be made and therefore it would be a huge waste of time – for me and for her.
Believing myths like the ones discussed here can prevent people from seeking therapy when they need it most. So it’s important to challenge these misconceptions so that people are informed and have an accurate depiction about what therapy is like. If you’ve been hesitant about therapy, remember: it is a tool for everyone! Taking that first step could be the start of the rest of your life and provide the transformation and growth that will turn your life around.
She ordered a skinny, zero sugar vanilla latte. I ordered a caramel latte – no ‘skinny’ or ‘sugar free’ in sight.
She said she worries that she’ll never get back to work, is sad that she is missing out on all the life experiences she was looking forward to because chronic illness is cruel. I said I agreed, but that at least she’d learn there’s life beyond an eating disorder.
I tell her that it’s ok to feel lost and alone – because it’s not a feeling that will last forever.
She tells me that she’s scared she’ll always feel like an outsider or that something is ‘wrong’ with her. I tell her that she’ll find her people. People who love her and understand her, and that she’ll finally learn there is nothing wrong with her after all.
She told me that she feels on edge and frustrated whenever she has to use a walking stick or wheelchair. I tell her it’ll become second nature and people won’t care about it.
She asked me if I believed that God has a plan for her life. And for the first time in a long time, I could tell her I did.
As February is Fowler’s Syndrome Awareness Month, I decided to find out what some common questions were that people have about Fowler’s, as well as asking others with the diagnosis what they wish they had asked when it was first brought up for them. One of the things I’ve been asked the most is ‘what is your fowlers story?’ but I’ve decided to leave this for a separate post for now as it’s pretty long!
What are the main symptoms and what were your initial symptoms?
The main symptom is an inability to urinate – this can either be a partial inability or full inability. Sometimes people may have to strain to empty their bladder, or take a long time to fully empty their bladder. Bladder spasms can be a huge issue for people with the condition as well.
Often, people are unable to feel when their bladder is full. I rarely have bladder sensation unless I have an infection (which is when I often feel like I constantly need to go to the toilet).
Stomach, bladder and pelvic pain are common side effects of Fowler’s. Pain can increase with specific movements and activities. Frequent infections can also exacerbate pain levels. Infection is also common – this can be because having a catheter is something that can increase susceptibility to infection, or being unable to fully empty the bladder can also increase the risk.
My initial symptom was a kidney infection – it sent me in to full retention. When it was treated the symptoms appeared to resolve, though it’s likely that I was in partial retention. I then went back into full retention again, and so this, along with increased pelvic pain, were my initial symptoms.
How is it diagnosed?
Fowler’s Syndrome is a difficult condition to diagnose, but the gold standard test is a specialist one called ‘concentric needle electromyography’ (an EMG). Abnormal electrical activity on this test signifies Fowler’s. It’s a pretty uncomfortable test as a needle is used to record from the sphincter.
Other tests that can be carried out include looking at flow rate, residual bladder volume scanning, urethral pressure profile, and ultrasound sphincter volume. However, these tests depend on whether you pass urine naturally or not.
Urodynamics are often the first test that is given as it is commonly carried out in urology departments – if you are in full retention it is unlikely that there will be any useful results, although it can show whether or not your detrusor muscle (the main bladder muscle) is functioning at all.
How long did it take for you to get a diagnosis? Are there any common misdiagnoses?
I was incredibly lucky to get my diagnosis within 4 months of the initial onset of symptoms. On average it takes people seeing 8 professionals before diagnosis and it can take years before a solid treatment plan is given.
The most commonly given first diagnosis is Detrusor Failure (Acontractile Detrusor) as this is a diagnosis that can be given after urodynamics which is the go to test for urological problems. However, when the EMG is done this then highlights the problem with the sphincter muscle and allows the diagnosis of Fowler’s to be given.
When it was first mentioned to you as a diagnosis/given as a preliminary diagnosis how did that make you feel?
In all honesty, I didn’t know what to think. I’d never heard of Fowler’s so it was a lot to get my head around. I didn’t know what to expect, I thought I’d need a catheter for a matter of weeks or months, and certainly didn’t expect to still have one 6 years later! But it was also a relief. No one was telling me that I was making it up or that they didn’t know why my symptoms had started, they could say ‘we might not know a lot, but we do know this’ and that felt reassuring at a time when I didn’t know what to expect next.
What treatments are there? What have you tried in the past? Are there any treatment options you hope to try in the future?
There isn’t a cure for Fowler’s but there are treatments that can be tried. Treatments are still being researched and developed.
The one that a lot of Fowler’s patients try is Sacral Nerve Stimulation – this is particularly good for patients who are in full retention. Those in partial retention may benefit, but their symptoms are more likely to respond to self-catheterisation in order to fully empty the bladder. SNS is the only treatment that has been shown to restore voiding in patients who are otherwise in full retention. In short, SNS is like having a pacemaker for your bladder – it sends electrical signals to your sacral nerves (the nerves that control the bladder). You usually have a trial first to see if it is effective enough and if it is then the full device is implanted.
A Suprapubic Catheter (SPC) is a surgical catheter that is inserted into the bladder through your lower abdomen. This can be better for those with Fowler’s as they bypass the urethra and so there are often fewer urethral spasms when a SPC is in situ rather than a urethral catheter.
Bladder botox has been used for years for people with overactive bladders. It has been used for Fowler’s patients and has shown improvements in bladder emptying for some, as well as reducing bothersome symptoms like spasms and pain. The botox is injected directly into the sphincter and is usually effective for between 3-9 months.
There are two more drastic options as well:
Mitrofanoff surgery is a form of urinary diversion. The purpose of this is to form a man-made channel between the bladder and abdominal wall to allow intermittent self-catheterisation through the abdomen rather than urethrally. Often, it is made using the appendix, but when this isn’t possible part of either the small or large bowel can be used. This option means that you don’t need to have a catheter permanently in place or be attached to a bag.
A Urostomy is a type of stoma and is another form of urinary diversion. A small section of bowel is used to form the stoma and this is connected to the ureters (the tubes that are connected to the kidneys). You then have a stoma bag that collects the urine and needs to be emptied throughout the day and changed regularly.
Both of these are options that are seen as a last resort due to the complexity of them and the recovery time that is needed.
I currently have a SPC (I’ve had it for 4 years now!) and have tried SNS but was told the trial wasn’t effective enough. I’m currently waiting to see if I can have another trial through pain management as it was very effective for my pain levels, and I should find out about this at the end of the month. I’ve been told by one consultant that Mitrofanoff or Urostomy surgery is my only option now, but this isn’t something that has been discussed further.
What is one thing you wish people knew about Fowler’s Syndrome?
That it is so much more than not being able to pee! It’s infections, sepsis, pain, leaking catheters, blood, more pain, spasms, medications, repeat hospital appointments, lack of understanding from professionals and those around you. It causes fatigue and can completely turn your life on its head. It’s a lot.
What is the hardest part about having Fowler’s Syndrome?
For me, it’s the catheter. I have very specific reasons why this is difficult – I have C-PTSD and my catheter is a huge trigger for me and so I find it incredibly hard to live with a catheter that causes such difficult emotions and thoughts to come up. I find catheter changes incredibly difficult because of this and it made self-catheterising near on impossible for me.
Have you had any positive experiences with medical professionals about it, and if so, how has that impacted you?
I have! My first urology nurse was incredible. She was very empathetic and understanding, and I really felt listened to by her. She is actually the reason I started sharing my journey more openly. I had spoken to her about how I felt like I must be the only person in the world my age to be experiencing symptoms like I was, and she sat me down and told me that it was so much more common than people thought. She said she’d love there to be a young urology ‘poster-girl’ (as most leaflets I got given featured pictures of old people on them) and it was after that appointment that I decided to open up more and raise as much awareness as possible.
I’ve also been really lucky to have some incredibly district nurses coming out to me for catheter changes. They’ve held my hand, reassured me when I’ve had flashbacks, stayed at my flat for far longer than they should in order to make sure that I’m ok after a change. They’ve had cups of tea with me and listened to me play the piano, told me about their lives – treated me like a human and not a number. They’ve let me get to know them as much as possible so that I really feel like I have trusted relationships with them, which due to past trauma is something that means a huge amount for me.
If you could change just one aspect of Fowler’s Syndrome, what would it be?
The pain. Definitely the pain. I think I could come to terms with the catheter if I didn’t have to put up with such debilitating pain and spasms.
If you could speak to med students, what is the most important thing you would want them to take away from the conversation?
I actually spoke to some med students about Fowler’s last year! I was an inpatient on a psych ward (so I doubt they were expecting me to start talking urology at them) and they asked if they could have a chat with me and listen to my story. I told them that if there was one thing I wanted them to take from our discussion it was to remember what Fowler’s Syndrome is and to share it with fellow med students and lecturers. I appreciate that it is a rare condition, but it has such wide reaching effects and it still deserves attention and awareness.
If anyone ever has any questions about Fowler’s Syndrome or bladder health in general, I’m always open to answering anything you want to know about!
Living with chronic illness is a journey that is full of challenges – physical, emotional, social – you name it, it can be a challenge. Among these, loneliness is something that is incredibly common but is also underestimated by a lot of people. Chronic illness fundamentally reshapes your entire life – activities that one brought you joy may no longer be possible due to pain or fatigue, friends and family may struggle to understand your limitations which also leaves you vulnerable to feelings of loneliness.
Social events often require energy and effort that a lot of people with chronic illness are unable to participate in. Spoon theory is a good way to describe the energy limitations that are imposed on someone with a chronic health condition, and often we simply lack the ‘spoons’ needed. This can lead to feelings of isolation as being around friends and family is how we feel connected and is something that people need – we use solitary confinement in prisons as a punishment because it removes that connection that all humans need.
As well as this, when people misunderstand our illness or limits that we have, it can lead to a lack of empathy or patience. It’s understandable that, unless you’ve got a chronic health condition yourself, you can’t fully comprehend what life is like. And as chronic illnesses are so unique and symptoms vary drastically from person to person there can be misunderstanding between individuals with the same condition. It often feels like no one understands what life can be like, and this is a lonely place to be!
Loneliness doesn’t just stem from chronic illness either – it can actually worsen it. Social isolation can exacerbate feelings of depression, anxiety, and hopelessness, which can, in turn, amplify physical symptoms. It can feel like a never-ending cycle that is impossible to break.
But despite the loneliness that you may feel, there are other ways to connect with people. I have found communities online that have allowed me to connect with and speak to other people with chronic illness who understand what life can be like. For me, social media is my connection to the outside world – if I didn’t have access to it then life would feel even more isolating for me. I sometimes take breaks from social media as it can feel overwhelming at times, but I do miss the sense of community and understanding when I am away from those groups.
If you know someone who is living with a chronic illness, remember that your understanding and patience can make all the difference. Reach out, listen without judgement, and offer support in whatever way your loved one needs. Offer to pop round for a cup of tea or to go to drop off some shopping. Ask if they want to chat on the phone or over facetime. Find out if they need help with jobs around the house and offer to go over and help them get some bits done. Whatever is needed at the time – knowing that they have people who love and care about them will undoubtedly make the person struggling with chronic illness feel valued and connected to you!
When I was diagnosed as autistic, I started to read (probably a little obsessively) up on the condition. I wanted to know everything and anything about it, and read about other people’s experiences as well. Here are some of my top books that I have come across!
To the outside world, Emily looks like a typical girl, with a normal family, living an ordinary life. But inside, Emily does not feel typical, and the older she gets, the more she realises that she is different. As she finally discovers when she is 16, Emily is autistic. Girl Unmasked is the extraordinary story of how she got there – and how she very nearly didn’t.
In this simple but powerful memoir, we see how family and friends became her lifeline and how, post-diagnosis, Emily came to understand her authentic self and begin to turn her life around, eventually becoming a mental health nurse with a desire to help others where she herself had once been failed.
Ultimately uplifting, Girl Unmasked is a remarkable insight into what it can be like to be autistic – and shows us that through understanding and embracing difference we can all find ways to thrive.
In 2021 Ellie was diagnosed with autism and ADHD and although it felt like the light had finally been switched on and she wasn’t just ‘broken’, the room before her was messy from a lifetime of being misunderstood. She quickly found that she wasn’t the only one, in fact 80% of autistic females remain undiagnosed at age 18 and only 8% of adults affected by ADHD have a formal diagnosis. Even with a diagnosis, most are left asking, what now?
Ellie’s mission is to change that. To challenge the common misconceptions about neurodivergent conditions that are preventing marginalised people get the diagnosis they need, and to provide simple, actionable resources so that they can live without the fear and shame that she did.
UNMASKED is Ellie’s kind and supportive guide that sheds light on everything from masking to the diagnostic process and from sensory overload to navigating the workplace, so that every reader can better understand themselves and others, and ultimately, make society more inclusive.
Laura James found out that she was autistic as an adult, after she had forged a career for herself, married twice and raised four children. This book tracks the year of Laura’s life after she receives a definitive diagnosis from her doctor, as she learns that ‘different’ doesn’t need to mean ‘less’ and how there is a place for all of us, and it’s never too late to find it.
Laura draws on her professional and personal experiences and reflects on her life in the light of her diagnosis, which for her explains some of her differences; why, as a child, she felt happier spinning in circles than standing still and why she has always found it difficult to work in places with a lot of ambient noise.
Have you, a friend or family member been living with undiagnosed autism?
For every visibly Autistic person you meet, there are countless ‘masked’ people who pass as neurotypical. They don’t fit the stereotypical mould of Autism and are often forced by necessity to mask who they are, spending their entire lives trying to hide their Autistic traits. In particular, there is evidence that Autism remains significantly undiagnosed in women, people of colour, trans and gender non-conforming people, many of whom are only now starting to recognise those traits later in life.
Blending cutting-edge research, personal insights and practical exercises for self-expression, Dr Devon Price examines the phenomenon of ‘masking’, making a passionate argument for radical authenticity and non-conformity. A powerful call for change, Unmasking Autism gifts its readers with the tools to uncover their true selves and build a new society – one where everyone can thrive on their own terms.
The modern world is built for neurotypicals: needless noise, bright flashing lights, small talk, phone calls, unspoken assumptions and unwritten rules – it can be a nightmarish dystopia for the autistic population. In Untypical, Pete Wharmby lays bare the experience of being ‘different’, explaining with wit and warmth just how exhausting it is to fit in to a world not designed for you.
But this book is more than an explanation. After a late diagnosis and a lifetime of ‘masking’, Pete is the perfect interlocutor to explain how our two worlds can meet, and what we can do for the many autistic people in our schools, workplaces and lives. The result: a practical handbook for all of us to make the world a simpler, better place for autistic people to navigate, and a call to arms for anyone who believes in an inclusive society and wants to be part of the solution.
During the first thirty years of her life, comedy script writer Sara Gibbs had been labelled a lot of things – a cry baby, a scaredy cat, a spoiled brat, a weirdo, a show off – but more than anything else, she’d been called a Drama Queen. No one understood her behaviour, her meltdowns or her intense emotions. She felt like everyone else knew a social secret that she hadn’t been let in on; as if life was a party she hadn’t been invited to. Why was everything so damn hard? Little did Sara know that, at the age of thirty, she would be given one more label that would change her life’s trajectory forever. That one day, sitting next to her husband in a clinical psychologist’s office, she would learn that she had never been a drama queen, or a weirdo, or a cry baby, but she had always been autistic.
A summary of my book:
1. I’m diagnosed with autism 20 years after telling a doctor I had it.
2. My terrible Catholic childhood: I hate my parents etc.
3. My friendship with an elderly man who runs the corner shop and is definitely not trying to groom me. I get groomed.
4. Homelessness.
5. Stripping.
6. More stripping but with more nervous breakdowns.
7. I hate everyone at uni and live with a psycho etc.
8. REDACTED as too spicy.
9. After everyone tells me I don’t look autistic, I try to cure my autism and get addicted to Xanax.
10. REDACTED as too embarrassing.
‘Fern’s book, like everything she does, is awesome. Incredibly funny, and so unapologetically frank that I feel genuinely sorry for her lawyers.’ – PHIL WANG
Ellie Middleton is back with a new, practical book to help you work WITH your neurodivergent brain rather than AGAINST it. In each chapter, she writes about the eight executive functions that neurodivergent people struggle with including working memory, prioritisation and emotional regulation and shares 5 simple tips for readers to try out, including:
– Creating a launch pad to remember the essentials when you leave the house – Drawing a car park of ideas to help visualise your thoughts and manage impulse control – The 5, 4, 3, 2, 1 mindfulness technique to prevent spiralling and regulate emotions – Breaking up each day into Four Quadrants to approach every day with more flexibility
This isn’t another journal or planner that claims to organize your entire life because Ellie is the first to admit that she doesn’t have things under control 100% of the time. This also is not a book about how to fit into the neurotypical way of doing things (aka masking). Instead, Ellie reveals why society tells us that we ‘should’ do things (read: patriarchy, ableism, White supremacy) and shows us how we can all free ourselves of those expectations, feel empowered and, ultimately, be more YOU.
Growing up, Chloé Hayden felt like she’d crash-landed on an alien planet where nothing made sense. Eye contact? Small talk? And why are you people so touch-oriented? She moved between 10 schools in 8 years, struggling to become a person she believed society would accept, and was eventually diagnosed with autism and ADHD. When a life-changing group of allies showed her that different did not mean less, she learned to celebrate her true voice and find her happily ever after.
This is a moving, at times funny story of how it feels to be neurodivergent as well as a practical guide, with advice for living with meltdowns and shutdowns, tips for finding supportive communities and much more.
Whether you’re neurodivergent or supporting those who are, Different, Not Less will inspire you to create a more inclusive world where everyone feels like they belong.
Written by two late-diagnosed neurodivergent women and the founders of fast-growing online community @IAmPayingAttention, HOW NOT TO FIT IN is an handbook-meets-rallying cry.
Foregrounding real experiences with autism and ADHD, this book explores the journey of discovering, accepting and flourishing with your neurodivergent brain. It explores why getting diagnosis can be so fraught and gendered, and how to navigate a world which centres neurotypical brains in the realms of relationships, careers, friendships and finances.
By reading this book, you’ll:
Start to understand why so many people are being diagnosed with ADHD and autism right now
Learn the impact that not knowing your own brain can have on your mental health
Find the confidence to ask for accommodations and adjustments at work – without apologising
Have the chance to note down how this journey is evolving for you in chapter-by-chapter workbook sections.
… and, most importantly, get to know yourself and your needs better.
Featuring the latest research and thinking on neurodivergence, contributions from dozens of experts and the real stories of people just like you, this innovative book – which has been written and designed especially for *spicy* brains – is essential reading for anyone whose brain seems to see the world in a different way.
In this ground-breaking debut, Charli Clement combines their own experiences alongside unique short profiles from individuals with chronic illness, to provide an intimate and insightful look at the complexities of living as an autistic and chronically ill person.
From navigating your diagnosis and healthcare, learning how to manage pain and your own sensory needs to dealing with ableism, medical misogyny and transphobia, Clement offers practical advice and delves into the unique challenges faced by individuals living in this intersection.
With a focus on the unique neurodivergent experience and an exploration into disability pride and joy ‘All Tangled Up in Autism and Chronic Illness’ is a necessary and empowering resource for autistic and chronically ill people as well as for family members, friends, and healthcare professionals.
I could go on and on about the books that I’ve read or heard good things about, but for now I’ll leave it at this. Happy reading!
Autism (or Autism Spectrum Disorder – ASD) is a neurodevelopment condition that impacts social interaction, communication, and behaviour. Whilst a lot of the research into ASD focuses on children, it’s important to remember that autism doesn’t just disappear with age – autistic children grow into autistic adults. Those with autism face unique challenges that can hugely affect mental health.
Adults with autism are at a higher risk of developing mental health conditions compared to the general population – it is estimated that between 70-80% of autistic individuals will experience mental health difficulties in their life. Common co-occuring conditions include anxiety disorders, depression, PTSD and OCD.
There are so many factors that can contribute towards mental health struggles:
Social isolation – many autistic adults struggle with building and maintaining relationships because they have difficulties in understanding social norms or managing in social situations due to becoming overstimulated. This can cause people to become isolated and increases feelings of loneliness, which is a huge risk factor for poor mental health.
Masking and burnout – masking is extremely common in autistic adults (with women being more likely to do this) as people try to suppress their autistic traits in order to fit in. This can help them to manage situations but in the long run it is exhausting and can lead to burnout with increased anxiety and depression.
Unemployment or underemployment – many adults face barriers to stable employment due to misunderstandings about their abilities or things like finding the work environment too overwhelming and overstimulating. This can lead to financial issues and impact self-esteem and feelings of worthlessness.
Sensory overload – when in an environment that is too loud, bright, or busy can overwhelm someone who is autistic, and this can cause long-term emotional and physical fatigue.
Lack of understanding and support – there is often a lack of empathy or accomodations and autism is still something that is very misunderstood. As well as this, when diagnosed in adulthood you are told that yes, you have autism, and may be offered a follow up session to discuss this, but then you’re on your own.
There are many ways that people can support the mental health of autistic adults – whether that’s support from other people, or support from yourself.
Build supportive networks – it can be helpful and beneficial to try and make connections with people who have similar experiences, and is definitely positive to try to form relationships with others who have a respect for neurodiversity and don’t see it as a negative thing.
Practice self-care and sensory regulation – you might need to spend time in quiet spaces, utilise things like weighted blankets, or sensory lighting as well as engaging in hobbies and activities that bring you joy. Making regular space for decompressing and relaxing can ultimately help you to avoid burnout and shutdowns.
Educate others – raising awareness of autism and mental health in both professional and personal capacities will help bring about more understanding and inclusion.
For far too long, autism and mental health have been stigmatised, leading many adults with ASD to feel invisible and misunderstood. By promoting neurodiversity barriers can be broken down and more and more people will come to understand that autism isn’t a problem to be cured or fixed, but a different way of experiencing the world.
Whilst mental health problems are not an inevitable part of living with autism, they are more likely as the world refuses to accommodate or understand neurodiverse needs. If you are an autistic adult, or someone who loves one, remember that seeking help is a positive thing – with the right support good mental health is more than achieveable!
Last year I was diagnosed with Autism. It was a diagnosis that had been brought up a few times in the past, but until recently I wasn’t open to the possibility of an assessment. I’d rather unpolitely told my key worker when I was under the Child and Adolescent Mental Health Service to stick it. But last year I had my assessment as I decided that I’d lived long enough feeling like something was wrong with me and I needed answers.
For so many people, myself included, being diagnosed as autistic can feel like that one missing piece of the puzzle has finally slotted in to place. It is a moment of clarity that can explain years of feeling different and misunderstood. But it can also bring about other emotions – relief, confusion, grief, and sometimes joy. More and more people are finding out that they’re autistic as adults as we finally recognise what autism looks like and how it might present. This comes after years of trying to navigate a world that wasn’t built for them.
ASD is a historically under-diagnosed condition especially in women, people of colour, and those who don’t have obvious behavioural challenges. Many of us who are diagnosed later in life grew up at a time when autism awareness was limited and only really associated with children or those presenting with stereotypical traits.
For me, I spent years of my life feeling like something was wrong with me. I never seemed to fit into the typical mould that my peers did – I wasn’t interested in the same things as them, I preferred to spend time alone, and I really struggled with forming and maintaining friendships. So when I received my diagnosis I felt a huge wave of relief because there was finally an explanation for why I had felt different my entire life. It provided validation and allowed me to stop beating myself up for my difficulties.
I started to feel all the feelings – I felt sad, frustrated, angry and overwhelmed, with relief mixed in for good measure.
I was angry with myself that when CAMHS discussed the possibility of me being autistic, I told them to stick it and refused to discuss it any further. I felt angry with myself that I never went ahead with an assessment. I was frustrated that no one else noticed the signs prior to this, especially when everything began to feel incredibly obvious.
Why did I feel like this?
Because if I had been recognised as autistic 5, 10, 15 years ago I’d have probably achieved my degree. I’d have been able to understand myself better and make adjustments that may have made university and work more feasible. I might not have chronic mental health issues or have spent so long in environments that are so unsuitable for neurodiverse individuals. I’d have had years to wrap my head around it all. I began to feel like life could look so different for me.
But I also began to learn that autism isn’t something for me to fix. And I started to feel relief that at least I could start to make adaptations to my life that will benefit me from here on. I realised that I could start to embrace myself in an authentic way and that I could celebrate my strengths and skills.
Yes, receiving my diagnosis meant I had to make a huge shift in self-understanding. I had to begin unlearning societal expectations that I’d spent years trying to adapt to. I realised that my diagnosis didn’t change who I am – I have always been autistic and will always be autistic – and that is ok! I now get to try and build a life that allows me to honour my needs, strengths, and individuality.
Chronic illness doesn’t just affect you, the person experiencing it – it has a ripple effect that spreads out to family, friends, colleagues. Something that I know a lot of people struggle with is the feelings of guilt that can arise because of this. Guilt can stem from feeling like a burden, missing out on social or work related events, or needing additional help from others. While this is a natural way to feel, it can have a long-lasting impact on mental health and relationships.
There are numerous reasons that you might feel guilty when struggling with chronic illness. Often people describe feeling like a burden as they require more support with things like shopping, cooking, cleaning or even washing yourself. This leads people to feel badly about the amount of time and energy that is being spent on your care. The nature of chronic illness is that they are unpredictable. This can mean that you have to cancel plans last minute and therefore feel like you are letting others down. It can also impact family dynamics and impose limitations on what you can do in terms of work – both of these can cause guilt as you feel like you are disrupting people from living their life or not pulling your weight.
I think it’s important to remind yourself regularly that needing help from others doesn’t mean that you are weak or less valuable. Relationships are mutual and those closest to you want to help you in any way they can. It can help to talk about your feelings of guilt – it may not be obvious to others that you are feeling this way, and talking to them means that they can reassure you that they are happy to help. They say a problem shared is a problem halved, right?
Even if you can’t contribute to things in the same way that you did pre-illness, you can find other ways to show your support, care and appreciation for those around you. Chronic illness is not your fault, and guilt won’t change your circumstances. Think of all the brain space you might free up if you’re not constantly berating yourself for what you can’t do!
Having healthy boundaries can help prevent resentment and allow your relationships to blossom and thrive. Remind yourself frequently that letting other people help isn’t weakness or a sign that you are no longer independent – you can be independent and still ask for help.
Remember this: guilt is a natural response to the challenges of living with chronic illness, but it doesn’t have to define your relationships or self-worth.
The last time I was lucky enough to see Wicked on their UK tour – I treated myself to front row seats and loved every second!
It’s no secret that I love the musical Wicked – I’ve been lucky enough to see it 7 times and seen 5 amazing Elphaba’s and 6 incredible Glinda’s perform. I used to dream of performing in a West End pit orchestra (and still do if I’m being honest) and Wicked would definitely be my dream show. I absolutely adore every part of it.
When we think of Elphaba and Glinda, it is easy to see them as opposites. Elphaba, the misunderstood outsider stands in direct contrast to Glinda, the sparkling picture of popularity. But the truth is far more nuanced than this. I think everyone has an inner Elphaba and Glinda – often one side more pronounced than the other, but there nonetheless. They’re not just fictional characters; they are symbols, mirrors for the parts of ourself we often hide or struggle to embrace.
Elphaba: For the Misfits and the Rebels
Elphaba is for every person who has felt like they don’t belong, like they’re too much or not enough all at once. She is for the ones who see the world differently and refuse to accept it as it is. She represents the misunderstood, the outcasts, and the rebels who dare to question the rules.
She is for:
Every undiagnosed autistic girl who never quite fit in
Every child who was labelled “too much” for simply being themselves
Every loner who found refuge in books, dreams, or the stars
Every person who stood up for what’s right, even if it meant standing alone
Everyone who has learned to find power in the very things other people tried to shame them for
Elphaba reminds us that being different isn’t a curse – it’s a gift. Her story is a testament to the strength it takes to stay true to yourself in a world that demands conformity.
Glinda: For the Dreamers and the Evolving
Glinda, on the other hand, is for the ones who thought they had to play by the rules to be loved. She represents the perfectionists, the people-pleasers, and the dreamers who eventually learn that authenticity matters more than appearance.
She is for:
Every girl who thought fitting in was the only way to matter
Every person who hid their insecurities behind charm and a dazzling smile
Every perfectionist who learned that growth comes from vulnerability
Everyone who discovered that true power lies not in being adored, but in being brave
Every friend who realised that love isn’t about staying the same, but growing together
Glinda shows us that it is never too late to rewrite your story. She reminds us that even the most sparkling facade can hide a heart searching for something real – and that transformation is possible.
Elphaba and Glinda teach us that there is no single way to be strong, no one path to belonging. Elphaba’s defiance shows us the power of staying true to ourselves, while Glinda’s evolution reminds us that growth and change are part of the journey. Together, they challenge us to embrace both our shadows and our light, our flaws and our potential.
Whether you see yourself in Elphaba’s fierce independence, or Glinda’s journey to authenticity – or perhaps a little of both – their stories are for all of us. They remind us that the labels the world gives us don’t define who we are. What matters is how we choose to rise, love, and grow despite them.
So, who are you today? The rebel standing tall against the storm? The dreamer learning to let go of perfection? Maybe, like Elphaba and Glinda, you are a little bit of both – and that’s where the magic truly happens.
I’ve written about the grief that accompanies chronic illness before, but it’s a topic that I often come back to because it is something that has been so prevalent in my life.
Living with chronic illness often comes with a deep sense of loss. It isn’t just the physical symptoms that affect your day-to-day life, but also the realisation that the life you imagined for yourself might never come to fruition. This feeling of loss can manifest as grief, a complex emotional process that many people with chronic illness experience.
Grief isn’t just something that is limited to the death of a loved one. People often grieve the loss of:
Physical abilities – the things you once took for granted like running, dancing, walking, might now feel or become impossible.
Independence – it’s hard when you have to suddenly rely on other people for help doing tasks that you would have previously handled independently with no problems. This is something that can feel incredibly vulnerable.
Future plans – you might have to give up on career goals, travel plans, or family aspirations, or at the very least, adjust your expectations of what you can realistically manage.
Sense of identity – chronic illness can force you to redefine who you are and how you see yourself. This is something that I have struggled with a lot – who am I without the things that I can no longer do. Who am I if I’m not studying or working?
Grief doesn’t follow a linear pattern at all. There are stages of grief that people go through but the order and time it takes varies massively from person to person. The five stages that people are said to experience are as follows:
Denial – “This can’t be happening to me.” You might ignore symptoms or resist a diagnosis.
Anger – “Why me?” It is completely natural to feel frustration and resentment about your situation!
Bargaining – “If I do everything that the doctors are telling me to do, maybe I’ll get better.” This stage also often involves clinging on to the possibility of a cure or treatment that will make life bearable.
Depression – “What’s the point?” Sadness and hopelessness can feel incredibly overwhelming.
Acceptance – “This is my reality but it doesn’t have to define me.” Accepting your situation doesn’t mean that you like your situation, rather that you are finding ways to move forward despite your diagnosis and struggles.
So, what can you do help cope with these feelings of grief?
You should allow yourself to feel your feelings. Don’t try to bury them because this isn’t going to help and will likely make things more difficult in the long run. It can also help to connect with other people who understand what life with chronic illness is like – I’m very lucky to have found communities on Facebook and Instagram that have allowed me to meet other people in similar situations to myself.
Therapy can also be a very helpful tool. I have been seeing a counsellor for 4 years and she has been my lifeline, offering me a safe space to explore my feelings around my illness. Through therapy I have learned how to be more compassionate towards myself and to respect my body’s limitations. I now respond with kindness when I’m having bad days as I’ve learned that punishing myself is not going to be beneficial.
Grief doesn’t mean giving up – it means making space to acknowledge your losses but also the new opportunities that might arise as a result. Chronic illness may alter your life dramatically, yes, but it doesn’t erase who you are as a person. And it doesn’t have to get rid of your potential for growth, connection, and happiness.
Three years ago Dr Alex George decided to post a picture of himself holding the medication that he takes for his mental health. The idea behind it was to challenge the stigma around medication and mental health. When he first started taking medication he felt ashamed – a feeling that so many people have felt at the prospect of needing medication to help manage their mental health. Since then thousands and thousands of people have also joined in, posting pictures of their medication on the 1st of every month in an attempt to help remove the shame and stigma associated with meds.
I used to think that taking psychiatric medication was something to be ashamed of. I worried it made me ‘weak’ or demonstrated that I wasn’t trying hard enough. There was a part of me that believed that I should simply ‘push through’ and try to manage on my own. But here’s the truth: there is NO shame in taking medication for your mental health. Those thoughts that I had were planted by a society that still stigmatises mental health struggles and the tools we use to manage them.
When someone needs glasses to see clearly, insulin to manage diabetes or an inhaler because they have asthma, there is no hesitation. We simply accept that they need medication to help. So why is there so much stigma around mental health medication? Your brain is just as much a part of your body as any other organ and, sometimes, you need extra help.
Psychiatric medication doesn’t change who you are as a person. It doesn’t erase your personality or take away your emotions. It simply helps to create space for you to be more yourself.
Medication for mental health is just a different part of the ‘toolkit’ you can use to manage your mental health, just like talking therapy is a different way to benefit yourself. It doesn’t get rid of your struggles or do the work for you, but it does help make things more manageable. It can clear the fog long enough for you to engage in support like therapy and to help you implement the tools that you need in your day-to-day life. For some people it is medication that can get you to a point where you can get out of bed in the morning. For others it helps to lessen the anxiety that you feel or to manage unwanted thoughts and feelings.
It’s not a perfect process by any stretch of the imagination either. Finding the right medication and dosage can take a long time – I tried 11 different medications at various doses and for varying lengths of time before landing on a combination that works for me. I still struggle, and it doesn’t really help lift my mood much, but it definitely helps prevent me from hitting rock bottom. And choosing to explore the option of medication and being open to the possibility of taking meds isn’t a failure, it’s another way of saying “I deserve to feel better, and I am willing to try whatever it takes.”
Meds don’t come without potential complications, either. They can make things worse to begin with, and they take a while to fully kick in. There are also potential side effects to contend with (and sometimes additional meds needed to combat various side effects) or withdrawals if you are coming off a medication you’ve taken for a long time. But by acknowledging that you deserve to feel better you are deciding that your mental health matters and that you are wanting to take care of yourself. This isn’t a sign of weakness – it’s a sign of incredible strength.
If you’re on medication for your mental health, considering it, or simply curious about what it could do for you, remember this: there is no right or wrong way to look after your mental health. Some people find healing in therapy, some by exercising, some by taking medication. Often it is a combination of different approaches that can make the most difference. And if you’re feeling hesitant or alone because of the stigma, know that you are not alone. Here is what I wish I could tell my younger self:
Taking care of your mental health – however that may be – is an act of love. You are not weak. You are not broken. You are brave, resilient, and deserving of every tool available to help you live the life you want.
So, let’s keep talking about this. Let’s challenge the stigma and remind each other that there’s no shame in doing what you need to feel better. Because you – and your mental health – are worth it.
Every year, millions of people readily come up with New Year’s resolutions and are filled with anticipation that this might be the year that we eat better, exercise more, complete a project or achieve a life goal. And every year, by February (or let’s be real – by mid-January) planners are discarded, gyms are emptier and diets have gone out the window. Sound familiar? That’s because, for the most part, New Year’s resolutions are a load of crap.
They are built on a false premise – the idea behind New Year’s resolutions is simple: January 1st is some kind of magical reset that will transform you into a better version of yourself. But here’s the truth: change doesn’t care about the date on the calendar. There isn’t anything that special about the first day of the year. Waiting for a specific date to work towards achieving a positive goal or habit is just procrastination wearing a festive hat.
They set you up for failure – most resolutions are vague and unrealistic. They might sound nice, but without a concrete plan or measurable milestones, they’re destined to fail. When you inevitably fall short, you’re left feeling guilty and frustrated – not exactly the motivation you’re wanting, right?!
They’re all or nothing – resolutions are framed as black or white, there is no grey area. Either you’re hitting your daily step goal or calorie ideal or you’re failing. This is a recipe for disaster because life is messy and slip-ups are inevitable. It is not a reason to quit altogether.
They ignore the power of small, steady change – real, lasting change doesn’t happen in giant leaps; it happens in the small, consistent steps. Small wins help you to build momentum and, in turn, motivation. New Year’s resolutions are idealistic and built on the idea of instant transformation.
They’re driven by external pressure – lets be honest: how many resolutions you come up with are things you actually want vs things you think you should want. Unsurprisingly, when you make resolutions that are driven by what you think you should want, they become easy to abandon, and therefore fuel the feelings of guilt and failure.
They are a marketing ploy – New Year’s resolutions are a goldmine for companies looking to sell you something. Gym memberships, subscriptions to diet plans, apps that promise you productivity – they are capitalising on your hopeful (and usually short-lived) commitment to self-improvement. Instead of falling for the hype and buying in to something you don’t really want or need, ask yourself: do I really need this or am I falling for a clever sales pitch?
So, what’s the alternative?
Ditch the pressure-filled annual ritual and focus on a more sustainable approach to change – focus on habits and taking small steps each day, remember that you can start at any time because the best time to start is always now. Be compassionate and gentle with yourself and remind yourself that you can adjust your goals and plans as you need to. And, finally, make sure that your goals align with your values – you’re much more likely to keep motivated to achieve your goals if they fit who you are as a person!
The bottom line is this: you don’t need an arbitrary date or big resolution to grow or succeed. Real change happens gradually and consistently. I hope that the next year is the year where you learn to focus on building a life that feels good no matter what day of the year it is.
Content Warning: This post talks about suicide. Although no details are given please be mindful of this and don’t read on if this is something that might be triggering for you!
Have you ever had someone say to you, “It’s clearly not your time,” after a suicide attempt? If you have, you probably know how cliche it sounds. Those words can feel empty, as though they’re meant to close a conversation rather than open one. Yet, as much as I’ve resisted the phrase, I can’t deny the weight it holds in my own life. After surviving multiple attempts to die – despite every intention to leave this world – I’ve been forced to confront the possibility that those words might carry a truth I hadn’t been willing to see.
I’ve tried. Many times. In moments of despair, I’ve done everything within my power to end the pain. And every single time, something has stopped in from happening. Maybe it was an intervention of a friend, the police or hospital staff, or a twist of fate that kept me alive. Maybe it was sheer luck, or as I’ve come to consider more and more, maybe it was because it wasn’t part of the plan that God has for my life.
The idea that survival is part of a greater plan is as difficult to accept as it is to dismiss. If I believe that God has a purpose for my life – and some part of me does – then surviving when I was ready to die suggests that my story isn’t over yet. If my time had come, wouldn’t I have succeeded? Wouldn’t I finally have found that escape?
But believing in that purpose doesn’t make the pain vanish. If anything, it complicates things. I’ve found myself asking why God would keep me here, struggling, when I was so ready to let go. What possible reason could justify the agony that led me to those moments in the first place? It’s a question I don’t have an answer to – at least, not yet.
If you’re reading this, maybe you’ve asked yourself similar questions. Maybe you’ve also faced moments when death seemed like the only way out. And maybe, like me, you’re still here, unsure of why. Here’s the conclusion I’ve started to reach: survival might not feel like a gift in the moment, but it’s an invitation to keep going. To keep searching. To keep asking what’s next.
When I think about the times I’ve survived, I realise that those moments weren’t random. They were filled with small interventions – a text from a friend, a hug from a family member that I so desperately needed, the police turning up at exactly the right moment to stop me doing something I wouldn’t be able to undo. Those moments weren’t the answers to all my questions, but they were signposts pointing me toward something bigger.
Wrestling with God’s Plan
If you believe, as I do, that God has a plan for each of us, then the idea that “it’s not your time” takes on a heavier, more significant meaning. If God has kept me here through all of this, then it would stand to reason that my time to leave this world is not now – because if it were, I would be gone. Period.
But it’s hard to reconcile the pain and hopelessness that drive someone to attempt suicide with the concept of a loving God who is guiding everything. It can feel cruel. Why keep me here, God, if it hurts this much? Why not let me go when I was so ready, so certain?
I don’t know exactly what God’s plan for me looks like. But I’ve started to think that surviving is part of it. Being here, despite everything, is part of it. And maybe writing this, sharing this, is part of it too.
“It’s still clearly not your time” still sounds cliche to me. It probably always will. But maybe the reason it’s such a persistent phrase is because there’s a deep truth buried in it. If you’ve survived something you didn’t think you could survive, it’s worth considering that there might be a reason for that. Not in a shallow, sugar-coated way, but in a profound, weighty way that calls up to look deeper into our lives and our purpose.
So here I am, still trying to figure it all out. Still asking questions. Still frustrated. But also still here. And if you’re reading this, you’re still here too. Maybe that’s worth something. Maybe that’s worth everything.
‘But he said to me, “My grace is sufficient for you, for my power is made perfect in weakness.” Therefore I will boast all the more gladly about my weaknesses, so that Christ’s power may rest on me.” – 2 Corinthians 12:9
The festive season is a magical time filled with joy, love, and celebration. But for those living with a chronic illness, it can also be physically and emotionally taxing. The packed social calendar, financial pressure, and an expectation to be cheerful can feel overwhelming when your body is already having to deal with the daily challenges that chronic conditions bring. Here are some tips to help you navigate the holidays whilst prioritising your health and well-being.
Set boundaries early – communicate with your friends and family about what you can and cannot do. Let them know how your condition impacts your energy and availability.
You might want to plan shorter visits, especially if spending all day somewhere feels too much, a limited timeframe might work better for you.
You can say no without feeling guilty – declining invitations or skipping certain traditions doesn’t mean you’re ruining things, you’re just protecting your health.
Prioritise rest – the holidays are exhausting for pretty much everyone regardless of health issues.
Schedule downtime when needed.
Listen to your body – if you need to leave early or skip something completely then do that. Your body knows what it needs and should be respected!
Create a cosy retreat – somewhere where you can decompress where needed. I like to hide under fluffy blankets and put on my galaxy projector light and just *breathe*
Simplify your holiday plans to avoid unnecessary stress.
Delegate tasks – let other people help you with cooking, cleaning and shopping.
Embrace convenience – convenient options exist for a reason and they are there to be used! Do your shopping online, grab some microwave meals, scale back the festive decor – whatever works for you.
Prioritise your favourite traditions – focus on the things that bring you most joy. For me that’s a candle-lit carol service and trying to see at least some cool Christmas lights!
Stay warm and comfortable – winter weather can exacerbate symptoms for some people so take steps to stay cosy:
Layer up – wear comfortable, warm clothing, especially if travelling.
Heat therapy – use heated blankets/heat-pads or warm baths to soothe pain.
Hydrate – don’t forget to drink plenty of fluids.
Prepare for social interactions – family gatherings can be overwhelming places, especially if you’re trying to manage symptoms.
Plan conversation boundaries – be ready with a response if someone asks you intrusive questions about your health that you don’t want to answer (it’s okay to tell people you don’t want to talk about things!)
Bring your essentials – medications, snacks, TENS machine, headphones… anything you might need!
Take breaks – excuse yourself for some time to wind down if needed.
Mind your mental health – the holidays can be emotionally draining, especially if you’re unable to participate fully due to illness.
Practice self-compassion – remind yourself that it’s okay to have limitations and that you’re doing your best.
Stay connected – if you can’t physically go to gatherings, find ways to connect virtually if you can.
Seek support – reach out to any mental health professionals involved in your care if needed, speak to your GP, family or friends to share how you’re feeling.
Have a backup plan – chronic illness is unpredictable at the best of times! Create contingency plans for if things flare up.
Keep your activities as flexible as possible – if you don’t need to book things, don’t book them (I still haven’t been able to book the activity my sister planned for my Christmas present last year as I can’t reliably manage plans) and let loved ones know that plans might have to change if you’re not well enough.
Stock up – make sure you have enough medication for whilst pharmacies are closed/post might take longer, keep easy meals/snacks in, and any other essentials you might need.
Celebrate in your own way – sometimes, the best way to celebrate Christmas is to tailor it to your own needs.
Host a quiet celebration (if you’re well enough) – create a calm space with a few loved ones, that way you can tell them to leave when needed and be in your own space which might be more comfortable.
Focus on small joys – the hot chocolate, watching Christmas films, watching twinkling Christmas tree lights.
Remember the spirit of the season isn’t about doing everything, it’s about finding moments of peace and connection.
Christmas with a chronic illness can look different, but it can still be meaningful and joyful for you and those close to you. It can still be a time of cosy comfort and love, just on your terms – just remember to look after yourself and prioritise your boundaries as well as turning to others for support when needed!
If there’s one thing you read in its entirety today, please let it be this.
It been 2 year ago now since I knocked on death’s door! I went from being at a farm swap one day, to dying the next. It wasn’t a rare medical condition that brought me from being a healthy woman to a dying one either. It just hit hard, it hit fast and it would turn my life upside down.
In August of 2022 I had sepsis. And then in October of 2023 it came back. The goal of 2024 is to not get sepsis!
Before I had sepsis, I knew that sepsis was your body’s reaction to infection. I just thought old people got it or those with poor health. I didn’t know people like me(or that even my children) could get it so quickly and I didn’t know that sepsis had long term health affects. I was pretty uneducated about what sepsis was.
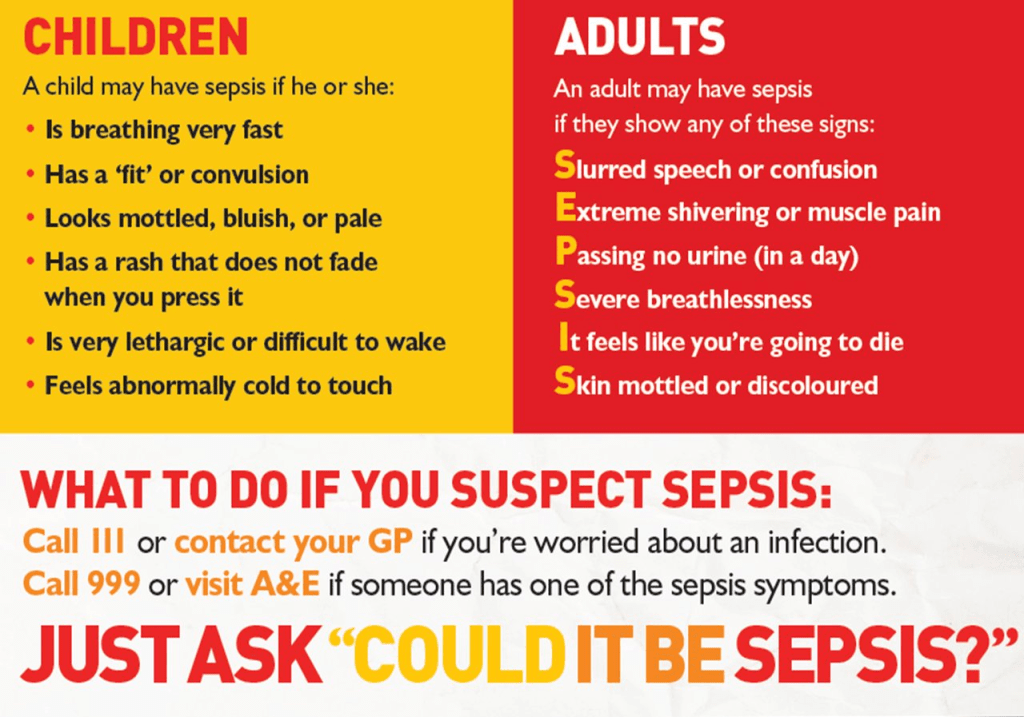
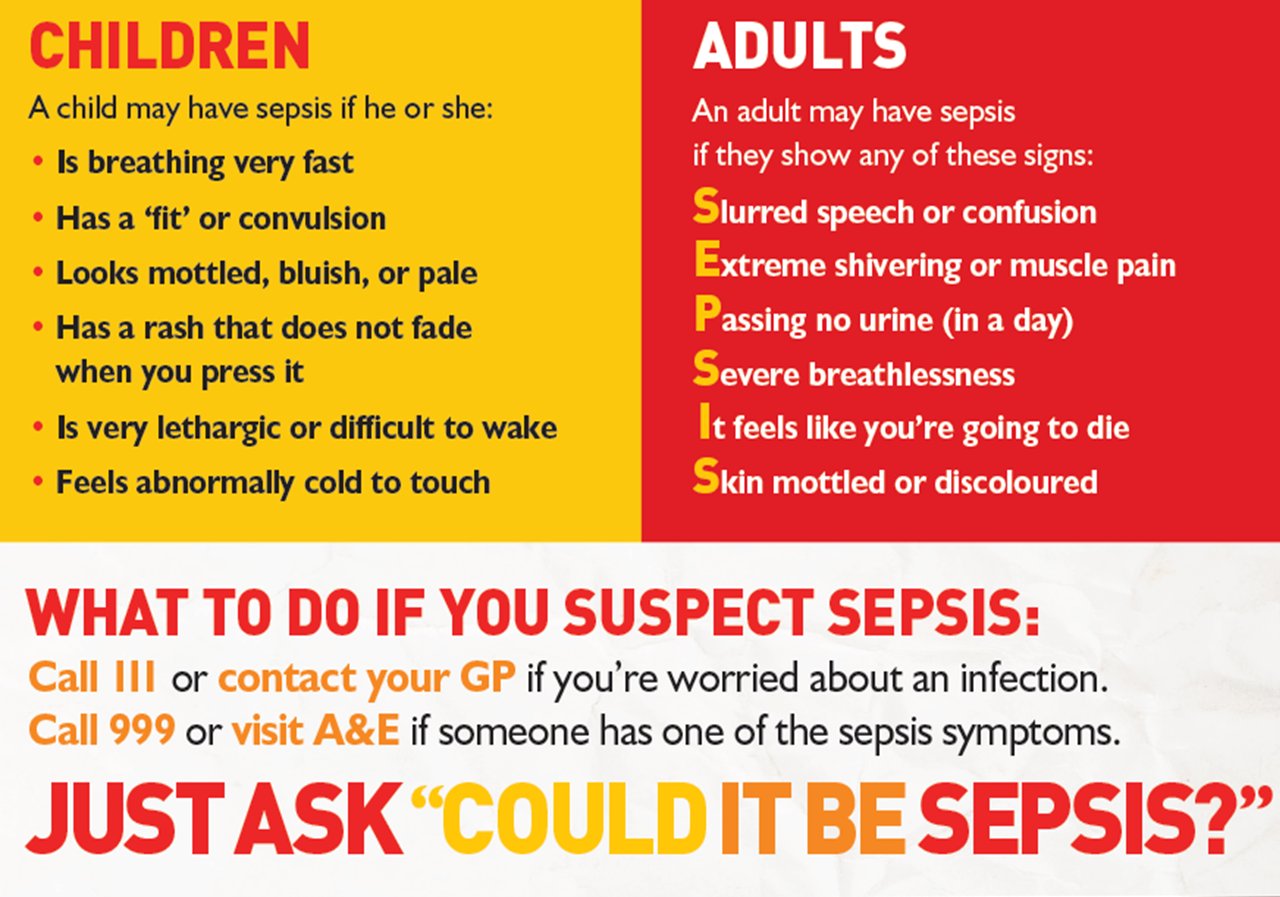
And so it’s become important to me to share what sepsis is, to tell you how to recognize signs of it and to tell you what post-sepsis syndrome is, in hopes that if you are sick you don’t wait to seek medical attention.
Sepsis is the body’s extreme response to an infection. If you don’t get treatment for it, it can lead to organ failure, tissue damage and death.
Symptoms of sepsis are not specific. They can vary from person to person. Initially my blood pressure was low and I had change in mental clarity… my mental state was the most drastic actually. So much so that the hospital ER staff believed I was high on narcotics and was treating me as such. It wasn’t until the hospital made contact with my husband and my best friend arrived at the ER that they were able to ensure the hospital I wasn’t a drug addict and that something else was wrong. And it was! I was finally given a urine drug screen and passed, but the long wait in the ER and being treated as just another addict had delayed much needed treatment and my sepsis turned into septic shock. My best friend saved my life that day.
I spiraled quickly… my blood pressure was low, my respiratory rates were high, I had a fever, I was hallucinating, I was shivering, I lost control of my bladder functions, I felt nauseous. I felt absolutely horrible.
Having sepsis led to my long admittance to the hospital. If I had stayed home, I wouldn’t have made it. If the hospital had delayed longer, I wouldn’t have made it. When people don’t get treatment, sepsis is a leading cause of death. Sepsis ranks higher than breast cancer, lung cancer, and heart attacks. It’s serious stuff. Sepsis can kill an affected person in as little as 12 hours and now that I’ve “been there, done that”, I can testify that this is absolutely true. I was feeling pretty deathly pretty rapidly.
Sepsis is treated with a strict antibiotic regimen. The underlying cause of sepsis or the original infection isn’t always known. It wasn’t ever clearly determined what caused me to get sick. They just have theories.
When I was discharged from the hospital I left knowing I’d be out of work for a bit, taking time to feel better, get rested, etc. But as the days grew to weeks, I wasn’t getting better. I found myself lost(literally), easily confused, at a loss for words, extremely tired, and unable to do tasks I once could. I would wake up and be disoriented to where I was. I’d sit in the house and not know what I was supposed to be doing. I’d try to do simple tasks like pickup dinner at the store and then completely forget why I was there. I would see people and they would act like we knew each other but I had no memory of them. Jason would tell me who they were but it’s like they never existed. I’d relearn people, names, and events. I would later find out that I had post-sepsis syndrome.
Post-sepsis syndrome affects 50% of sepsis survivors. Symptoms vary from psychological to physical effects. My short term memory was heavily impacted as was my cognitive functioning, similar to that of a traumatic brain injury. I had extreme fatigue and chest pains. My once normal heart now had tachycardia.
Post sepsis has required me to take medications just to stay awake during the day and to stimulate my brain. It’s changed my heart functioning and I take medications to keep it beating the right way. It’s made me forget some moments I desperately want to remember. It’s made simple memory tasks into harder ones. It’s made me rely on others to help do tasks I once could easily do. It’s enrolled me in rehab where we practiced skills to help my injured brain.
Now I do things on my speed and with tons of support from my husband and kids.
If you say “wow! I didn’t know!” It’s because I have the best support system someone could ask for. You don’t see me fail because of them. I succeed because they are behind me filling in the gaps.
I don’t share this because I want prayers or good vibes. I don’t want sympathy. On my two year almost dying anniversary, I want you to take sepsis seriously. Very seriously. I want you to go the doctor when you have an infection. I want you to take 5 mins today and to Google sepsis and read about all the signs and symptoms of sepsis.
I had a brainwave a couple of days ago and thought it would be really good to share as many stories of sepsis as possible on this platform. I might not have the widest reach in the world, but I have had people reading from across the world and sepsis is so serious that to me, it feels like a no-brainer. Awareness saves lives. I just want to thank every person who has agreed to share their story with me as it takes a lot to put yourself out there. Over the next couple of weeks I’ll be sharing various stories – please read and show some support to these amazing humans for wanting their story out there to hopefully help others!
On Saturday, September 2, 2017, I delivered a healthy baby boy and I was the happiest woman on earth. My husband and I had prayed for this child for years and this was going to be the start of our new adventure. What I did not know then was that this adventure was going to have a very rough start, one that still leaves me with nightmares.
On the day I was supposed to be discharged from the hospital I began to feel sick. I began to experience fever, chills, overall feeling of weakness, became short of breath, and felt like my heart was racing. I told my doctors all of my symptoms, but was quickly brushed off and was told that I was likely “just anxious about being a new mother.” Some tests were run and my White Blood Cell (WBC) count was higher than the previous tests, but again I was brushed off and told, “An elevated WBC count is normal after child birth.” When I was shivering from my fever, I was told to take a hot shower and one doctor even turned the thermostat in my room up to 80 degrees to stop the shivering. When my fever turned to sweats a nurse brought me a fan, again I was not taken seriously. Over the next few days I would continue to complain to doctors, but I continued to be ignored. One doctor even told me I was being “crazy” and needed to “stop”.
After doctors had given me enough Ibuprofen to make my fever go away for a while, they told me my new mom anxieties would likely go away when I got home and they sent me home with a prescription for anxiety medication. Not being a medical professional, or knowing what an elevated heart rate, fever, and elevated white blood cell count meant, I naively believed the doctors, that I would feel better once I got home.
Upon going home my symptoms did not improve. I continued to take the prescribed medications, including the anxiety medication prescribed by the doctor. My heart continued to race and I could not sleep or care for my newborn baby. Within about 36 hours of being released from the hospital, I couldn’t take it anymore and returned to the hospital first thing 9/08/17. On the way to the hospital I told my mother about the doctor telling me I was “acting crazy”, and was second guessing going back for fear that I would be told the same thing and sent home again. I am thankful my mom kept driving and insisted I get checked out. After a short stay in triage I was admitted into the hospital due to suspicions of an infection. Over the next 24 hours in Labor and Delivery my condition did not improve, I got progressively sicker and sicker as each hour passed. I went to the hospital to get better, instead I laid there getting worse. The OBGYN doctors had no real answers for my family. In the early morning hours of 9/09/17, I was finally taken to the ICU by a nurse from a different department who looked at my labs and knew something was extremely wrong. Had he not taken quick action, there is no doubt I would not have survived another 24 hours in the Labor and Delivery unit.
Over the next 2 weeks I would be treated for sepsis, endomitritis, septic shock, and all the other issues that go along with those, I.E.. kidney failure, shock liver, unstable blood pressure, pulmonary edema, blood clots, and the list goes on. I don’t remember much from my 9 days in the ICU and my earliest memories of waking up from my medically induced coma are filled with nothing but confusion. Where was my son? Did I even have a baby? Was that a dream? Whose hand did I trace the letters “C-R-U-Z” in to when I had a tube in down my throat?
I would later learn that was my mother’s hand that I traced my son’s name in to and that was one of the very first things I did when I woke up. As I started to become more aware my family and doctors carefully tried to explain to me that I had developed an infection of an unknown source. That was the very first time that I had ever heard the word, “sepsis.” At the time, I had no idea what septic shock even meant. I was very confused. I had no idea that I had literally just escaped death. I had no idea that during my time in ICU the doctors told my family to call those closest to me to say their goodbyes. I had no idea that my husband had to think about how he was going to raise his son without a mother. I had no idea that my son came so close to growing up without his mama. I had no idea what I had survived had killed so many others.
My husband recently visited another hospital in our area and noticed several posters about the symptoms of sepsis and we all talk about how if we had seen that information what might have been different. I constantly find myself saying, “I wish I had known about sepsis.”
Although my story of being a new mom got off to a rough start, today I am a happy, healthy, mama to a silly, smart, and sometimes a bit of a wild child boy. On the days when I get upset about missing out on the first month of dirty diapers, midnight feedings, and sweet baby cuddles I am reminded that not all who experience sepsis are as lucky as me. Now more than ever, I hear stories about people who have lost limbs, had severe long-term problems, and even died from sepsis. Throughout my one month stay in the hospital I constantly heard from medical professionals how “rare” sepsis is, but as I have done more research I am realizing sepsis really isn’t rare at all.
As I continue to share my story I find people just don’t know what sepsis is. I try to stress to everyone that while my sepsis experience was related to child birth, sepsis can affect anyone from something as small as a cut on your finger.
My goal in sharing my story is to help educate others about the symptoms of sepsis and the importance of advocating for your own health or the health of those around you. Because sepsis can affect anyone I want to help raise awareness across all audiences, but my experience has led me to have a special place in my heart for mothers-to-be. I I hope that more OBGYN teams will educate themselves on sepsis so that no family has to go through what mine did and even more so, I hope that pregnant women learn the symptoms and stand their ground if they feel that something is not right.
In January this year I had sepsis and it was the most terrifying experience of my life. It wasn’t the first time I’ve had it but it was the worst. As people with Fowler’s Syndrome are at higher risk of infections due to catheters, it follows that we are also at higher risk of developing sepsis. I’m really fortunate that because I was already in hospital at the time, it was caught early because things could have been much worse.
On New Years Eve I started to feel incredibly unwell. At first I thought it might just be the start of a migraine because I’m often sick and more exhausted than normal when I feel one coming on. But when the nurse in my bay came to do my observations I could tell something was seriously wrong. She immediately went to call a doctor and within 5 minutes my bed was surrounded.
My blood pressure had absolutely tanked (my notes, which I later read, said that it was 61/30), my temperature was 41°c and despite being in bed my heart rate was 149bpm. My score on the National Early Warning Signs system was 12. They took bloods straight away, including blood cultures, and put me on continuous fluids. And when they looked at what my lactate level was they knew that they were probably dealing with septic shock. A normal blood lactate level is less than 2.0mmol/L (some sources say that it’s less than 1.0mmol/L) and mine had jumped to 23. My entire body felt like it was on fire and I was beginning to feel quite disorientated.
Whilst they waited for my blood cultures to come back I was put on 3 different IV antibiotics until they knew what one was most appropriate. The critical care outreach team came to see me and discussions were had about whether or not I needed to be moved to intensive care. I wasn’t tolerating my feed at all so it had to be stopped for a few days, and when I woke up on New Years Day, I had the worst headache I’ve ever experienced. If I thought the headache that was starting the day before was bad, it was nothing in comparison to this.
I genuinely felt like my head was going to explode. I couldn’t move at all – I couldn’t sit up, turn from side to side, and the bright hospital lights just made everything worse. This made the medics suspect that I might have meningitis, but once my blood cultures came back, they realised that it was ‘just’ being in septic shock. I’m pretty glad that I didn’t have to have a lumbar puncture – I was hours away from that being carried out.
The continuous IV fluids were carried on until my blood pressure had stabilised a little – it took 4 days before it was normal enough that I was allowed to stand up and walk to the toilet (that was about 5 steps in front of my bed), and the same before my temperature dropped below 40°C. The critical care outreach team came to see me 4-6 times a day whilst my NEWS was still so high.
I don’t think I’ve ever felt so unwell in my life. All I asked the doctors for the first few days was ‘am I going to die?’ because I really did feel like that was the likely outcome. And now, being a science nerd who likes to read research papers for fun, it’s made things even clearer in terms of how unwell I was. In all honesty, the severity of my symptoms was probably also, in part, due to malnutrition and having experienced refeeding syndrome the week prior to going into septic shock. My body was struggling a lot.
It took a good 4 weeks before I started to feel semi-human again (although I still wasn’t at my baseline) and what did my body reward me with? Sepsis take two. I wasn’t quite as unwell the second time around, which I’m very grateful for, but it’s still taken it out of me. I’m still not back at baseline, even 6 months later, and I’m anticipating a long road ahead of me, but I know I’m incredibly lucky to be in the position I am, because things could have been very different.
Hair loss is a hugely sensitive issue that many people face for so many different reasons. Sadly, the stereotype and first assumption that people seem to jump to is that if someone has lost their hair (particularly if they are female), is that it must be due to chemotherapy. Whilst this is an assumption that isn’t made in a horrible way, and people usually ask out of a sense of compassion, it’s hard facing the questions time and time again. I wanted to write this post because I’ve lost count of the number of times I’ve been asked if I have cancer over the last 6 or so months (since my hair started to fall out again), and I feel it’s important to raise awareness of other conditions as well.
I have lost huge amounts of my hair in the last 6 months due to having sepsis.
So, what are some of the common causes?
Alopecia Areata: this is probably the most well-known cause of non-cancer related hair loss. It is an autoimmune condition that causes the immune system to attack hair follicles, leading to hair loss in patches. For some people, it can lead to total hair loss on the scalp, or even the entire body.
Genetics: male or female pattern baldness is hereditary. It can start as early as your 20’s and gradually lead to significant hair thinning.
Hormonal changes: hormones play a huge role in hair growth. Conditions like Polycystic Ovary Syndrome (which is coincidentally a condition that affects a vast number of those with Fowler’s Syndrome), thyroid disorders or the menopause can lead to hair loss or thinning.
Stress and trauma: this could be anything from major surgery or illness, to the loss of a loved one. Stress-related hair loss usually happens a few months after the triggering event.
Nutritional deficiency: if your diet is lacking essential nutrients like iron, vitamin D and protein, then this can contribute to hair loss.
Medications: not just chemotherapy – many medications can have hair loss as a side effect. These include blood thinners, many antidepressants, birth control and treatments for things like acne or arthritis.
Trichotillomania: this is a psychological condition where someone has an irresistible urge to pull out their hair, leading to noticeable bald spots. It is a form of compulsive behaviour and often needs professional help to overcome.
When people assume that hair loss equals chemotherapy and/or cancer (chemotherapy is also used for other conditions), it means that a vast number of other conditions are also being overlooked. And when people who have hair loss are repeatedly asked if they have cancer, it’s not only invasive, it also reminds them that there is something visibly different about them.
I, personally, have lost huge amounts of my hair this year due to having had Sepsis. The assumption is that because my body was so focused on fighting the infection, it took its energy away from bodily functions that it didn’t deem essential. I don’t hugely mind people knowing that I’ve lost my hair – I have, after all, posted photos clearly showing my hair loss. However, being totally transparent – I do find it hard when I go out without a wig because people have a tendency to point and stare at my head. When children ask questions I genuinely don’t mind answering them because I’d much rather educate others about why my appearance is the way it is, but it does take an emotional toll.
Next time you see someone dealing with hair loss, please try to resist the urge to jump to conclusions. Rather, offer them the compassion and respect that they deserve.
When we think about bladder health and urological conditions, the most common things that come to mind are things like UTI’s or incontinence. But there’s a much rarer condition that affects women (or those afab) – one that is often misunderstood, misdiagnosed, and far too frequently completely overlooked – Fowler’s Syndrome. Despite being something that is fairly unknown, Fowler’s can have a huge impact on quality of life, leading to physical pain, emotional distress and isolation.
What is Fowler’s Syndrome?
Fowler’s Syndrome is a urological condition that is characterised by the inability to pass urine normally. This is because the urethral sphincter (the muscle that controls the release of urine from the bladder) doesn’t relax like it should. It is a condition that mainly affects young women – especially those in their 20’s and 30’s. The exact cause is still unknown as well, and this only adds to the complexity and challenges of diagnosing and treating the condition.
The main symptom is urinary retention – the inability to empty the bladder properly. This is a spectrum with some people having mild difficulty in emptying their bladder, to other’s who are completely unable to empty their bladder without medical intervention. Many who have the condition will have to use a catheter to empty their bladder – either one that is permanently in situ, or by using intermittent catheter’s. Speaking from experience, both of these can be physically uncomfortable (and at times painful) and emotionally distressing.
Other symptoms can include:
Chronic pelvic pain
Recurrent UTI infections (the incomplete emptying of the bladder, or the presence of a catheter, leads to a higher risk of infections)
Lack of feeling in the bladder (I personally have next to no bladder sensation, even when I am totally at capacity)
Difficulty starting to urinate (even when the urge is strong)
A weak or slow urine stream
Diagnosing Fowler’s Syndrome is challenging. Because it is so rare, many healthcare professionals are not familiar with it and this can lead to misdiagnosis or delayed diagnosis. Women with the condition undergo multiple tests, including urodynamic testing which assess how well the bladder and urethra are functioning. One of the key symptoms (that is diagnosed by EMG – the gold standard test) is abnormally high urethral sphincter pressure, which prevents normal bladder function.
Living with Fowler’s Syndrome
Living with Fowler’s is not just a physical challenge, but an emotional one too. The daily discomfort and pain, needing a catheter, and frequent hospital and doctors appointments have a huge impact on mental health. Many women diagnosed with Fowler’s struggle with anxiety and depression as they navigate a condition that is not well understood, even by medical professionals (the consultant I was under after my diagnosis had never heard of Fowler’s and I was the first patient in the hospital to be experiencing the condition – it’s kind of scary looking back!)
There is also the challenge of explaining what Fowler’s Syndrome is to others. Because of its rarity, many friends, family, and doctors may not grasp what the person is going through. Those with the condition often have to become their own advocates, pushing for proper diagnosis and treatment options. I’m so fortunate to have the most amazing, understanding friends and family around me – I wouldn’t have gotten through the last 5 years without them in my corner.
Treatment Options
There is no cure for Fowler’s, but there are treatments that can help people manage the symptoms. The most common one is using a catheter to empty the bladder. As previously mentioned, this can either be through a catheter that is permanently in situ, or one that is used intermittently.
Another option is sacral neuromodulation – this involves implanting a device to stimulate the nerves controlling the bladder. This has shown promise in reducing symptoms for some, but it’s not suitable and does come with risks. It is thought to be less effective for those who are in complete urine retention.
Medications that relax the urethral sphincter or address underlying issues like chronic pain or mental health struggles may also be part of the treatment plan. However, because the symptoms are so individualistic and complex, finding the right combination of medications can take a lot of time.
Finally, there are surgical options but these are both huge undertakings. A mitrofanoff is a catheterisable channel that is on the patient’s abdomen that they then pass a catheter through to empty the bladder (or neo-bladder if one is created). A urostomy is where the urinary tract is diverted completely so urine drains from the kidneys to a stoma bag.
Why awareness matters
Fowler’s is rare, but for those affected it is a life-changing condition that definitely deserves more attention. Increased awareness can lead to earlier diagnosis, better treatment options and more research into potential treatment options and underlying causes.
Women with Fowler’s need to know they are not alone. They deserve understanding, support, and compassionate care. And I won’t shut up until everyone affected feels understood and supported through their journey.
Sepsis is the body’s extreme response to an infection. It isn’t the infection itself, but the reaction of the body that causes the problem. It’s a medical emergency that needs immediate attention, but for so many people it goes unrecognised until it’s too late. When your immune system goes into overdrive it can lead to tissue damage, organ failure and, if not treated quickly enough, death.
Imagine waking up one day feeling a little off. Maybe you think it’s the start of a cold or exhaustion because you’ve had a busy week. But as the day goes on, something starts to feel incredibly wrong. Your heart races, your breath becomes quicker, and all of a sudden, you’re hit with an overwhelming sense of confusion and fatigue. This isn’t just a simple illness – this is sepsis, something that can spiral out of control with alarming speed.
Knowing what to look out for is extremely important – sepsis is a medical emergency!
How might someone experience Sepsis and what is Post-Sepsis Syndrome?
For someone who has sepsis, the experience is terrifying and disorienting. It’s not just the physical symptoms you experience, but the mental disorientation and confusion, as well as an impending sense of doom. Often people are unable to think clearly, don’t know where they are or what’s happening, and they sometimes describe feeling like their body is shutting down.
And, even when someone is doing better, the journey isn’t over. For around 50% of people who survive sepsis they go on to develop Post-Sepsis Syndrome. This is something that can last for months, or even years after the initial infection. It is a collection of both physical and psychological symptoms that can have a huge impact on someone’s quality of life.
Physically someone might struggle with: fatigue, chronic pain, muscle weakness, organ damage, poor appetite, hair loss and shortness of breath. Psychologically the symptoms can include: hallucinations, panic attacks, flashbacks, anxiety, depression, insomnia, PTSD, nightmares and difficulty concentrating.
The risk of having PSS is higher for those who are either admitted to intensive care or are under an intensive care outreach team, and who are in hospital for a prolonged period of time. It is more likely that older survivors who have severe sepsis are likely to have worse cognitive and physical functioning post-sepsis. But it’s not exclusive to older adults – up to 34% of children are not back to their baseline for at least 28 days post hospitalisation.
Why is raising awareness important?
Sepsis is incredibly common – a lot more common that people may think. There are around 11 million deaths a year (with 48,000 people in the UK every year) and roughly 49 million cases of sepsis globally. It is thought to have a 20.3% death rate (according to a 2018 study) and, in the UK, nearly 80,000 people a year will suffer life changing after-effects. It also kills more than breast, bowel and prostate cancer combined.
However, despite being so common, and serious, people often underestimate the seriousness and prevalence of the condition. It’s very easy to think ‘I’m healthy, it won’t happen to me’, but the reality is that it can impact any one at any given time. I’m a strong believer that everyone should be educated on the symptoms of sepsis because delayed diagnosis leads to far worse outcomes. By raising awareness about sepsis, and PSS, it enables people to reach out for treatment sooner, and helps others understand what life post-sepsis can be like. The sense of isolation can be devastating, but there are people out there who do understand and who do want to help.
Sepsis is a life-changing condition that doesn’t end when you leave the hospital. So, spread the word about sepsis wherever you can. Let’s try to make a difference in the lives of sepsis-survivors, their friends, families and everyone who may experience sepsis in the future.